When filling out the Medication Administration Record Sheet, it's essential to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn’t do:
The Medication Administration Record (MAR) is similar to the Patient Medication Log, which serves as a comprehensive record of medications taken by a patient. Both documents track the administration of medications over time, ensuring that healthcare providers have a clear view of what has been prescribed and when it has been taken. The Patient Medication Log may also include additional details, such as side effects or patient-reported outcomes, which can enhance the understanding of a patient's response to treatment.
Another document that parallels the MAR is the Medication Reconciliation Form. This form is utilized during patient transitions, such as hospital admissions or discharges, to ensure that all medications are accurately documented and compared against the patient's previous medication list. Like the MAR, it aims to prevent medication errors and ensure continuity of care by confirming that patients receive the correct medications at all times.
The Treatment Administration Record (TAR) is also similar to the MAR. This document is often used in long-term care settings to record not only medications but also other treatments provided to patients. Both the TAR and MAR are essential for maintaining accurate records of patient care, and they help healthcare providers coordinate treatment plans effectively.
The Employee Handbook serves as a vital resource for employees, detailing essential information on company policies and workplace procedures. For a comprehensive understanding, employers may refer to additional resources such as the legalformspdf.com which provides valuable templates and guides related to employee handbooks.
The Nursing Care Plan shares similarities with the MAR as it outlines the specific medications and treatments a patient will receive based on their individual care needs. Both documents are integral to patient care, ensuring that nurses and other healthcare professionals follow the established protocols for medication administration and monitor patient responses accordingly.
The Prescription Record is another document that aligns with the MAR. This record details the medications prescribed to a patient, including dosage and frequency. While the MAR focuses on the administration of those medications, the Prescription Record serves as a foundational document that informs the MAR and helps track changes in medication therapy over time.
The Medication Administration Policy is also comparable to the MAR, as it outlines the procedures and guidelines for administering medications within a healthcare setting. While the MAR is a specific record for individual patient medication administration, the policy provides the framework that governs how those records are maintained and ensures compliance with regulatory standards.
Lastly, the Adverse Drug Reaction (ADR) Report is similar in that it documents any negative responses a patient may have to medications. While the MAR tracks the administration of medications, the ADR Report focuses on the outcomes of those medications. Both documents are vital for patient safety and contribute to the overall quality of care by identifying and addressing potential issues related to medication therapy.
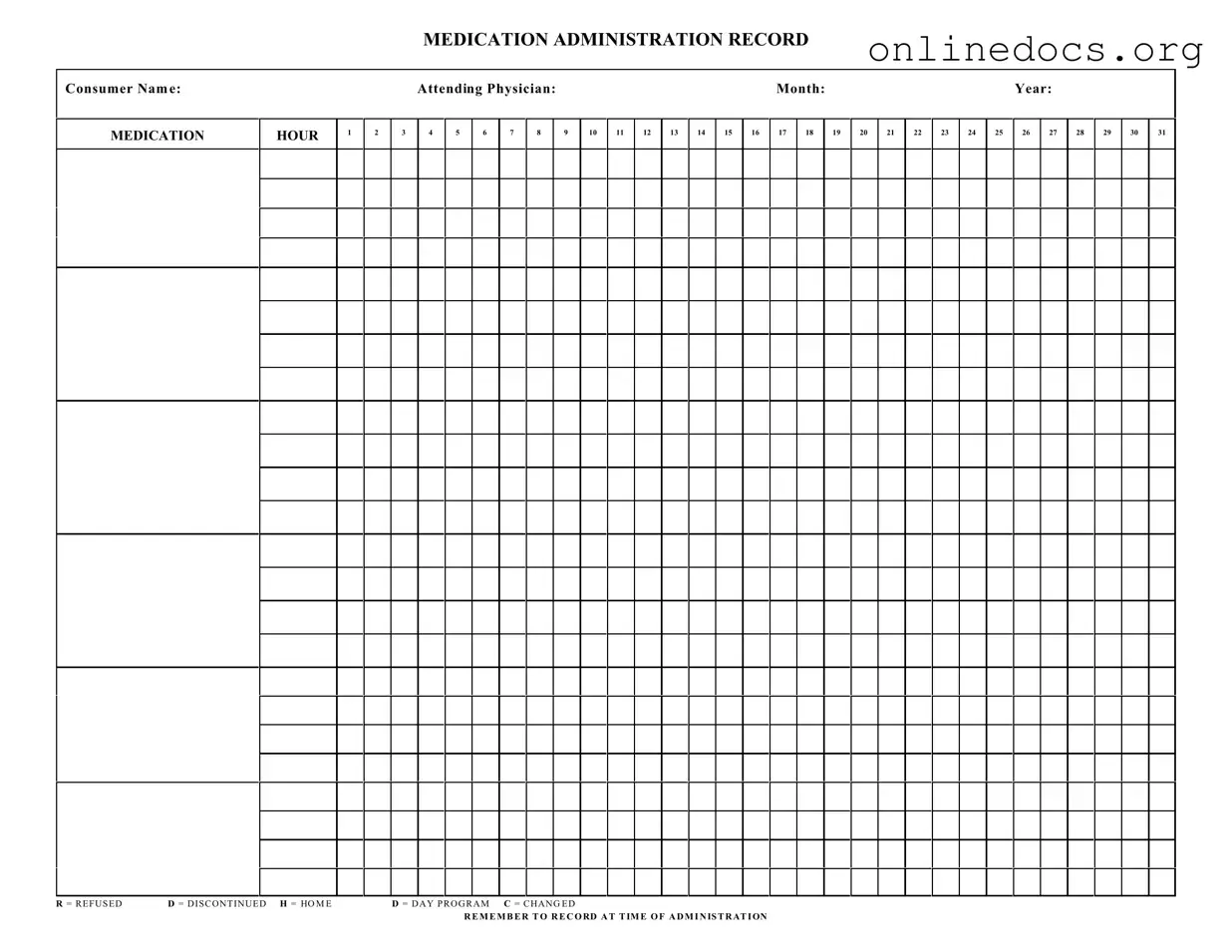
Filling out a Medication Administration Record Sheet (MARS) can be straightforward, but many people make common mistakes that can lead to serious consequences. One frequent error is not including the consumer's name at the top of the form. Without this essential information, it becomes difficult to track who received the medication, potentially putting patient safety at risk.
Another mistake is failing to record the attending physician's name. This detail is crucial for accountability and communication among healthcare providers. Omitting it may result in confusion about medication orders or changes in treatment plans.
People often forget to document the date accurately. Each entry should reflect the correct month and year. Errors in dating can lead to discrepancies in medication administration records, which can complicate audits and affect patient care.
Inaccurate time entries are also a common issue. Each medication must be recorded at the time of administration. Some individuals may write the time in the wrong column or skip it altogether, which can lead to misunderstandings about when a medication was given.
Another frequent oversight involves the use of the abbreviations provided on the form. Misunderstanding or misapplying these codes, such as R for refused or D for discontinued, can result in incorrect medication records. It's essential to use these abbreviations correctly to maintain clarity.
People may also neglect to update the record if a medication is changed or discontinued. Failing to note changes can lead to administering outdated or incorrect medications, which poses risks to the consumer's health.
Some individuals write down the wrong medication name or dosage. Double-checking these details is vital. Administering the wrong medication can have serious health implications.
Another mistake is not ensuring that all required signatures are present. Each entry should be signed by the person administering the medication. This signature provides accountability and can be critical in case of disputes or questions regarding the administration process.
Finally, many forget to keep the record legible. Handwriting that is difficult to read can lead to misinterpretations. Clear, neat writing is essential for effective communication among healthcare providers.
How to Get Proof of Dog Vaccinations - Customize with your clinic’s information and logo.
When establishing your business framework, it's vital to utilize a well-drafted customizable Operating Agreement template that specifies member responsibilities and procedures, ensuring smooth management of your LLC.
Pregnancy Verification Letter Planned Parenthood - Your emergency contact information is important to us.
Understanding the Medication Administration Record Sheet (MARS) is crucial for proper medication management. However, several misconceptions can lead to confusion. Here are seven common misunderstandings:
Clearing up these misconceptions helps ensure that everyone involved in medication administration understands their responsibilities and contributes to safe practices.